| Type
1 |
Type
2 |
|
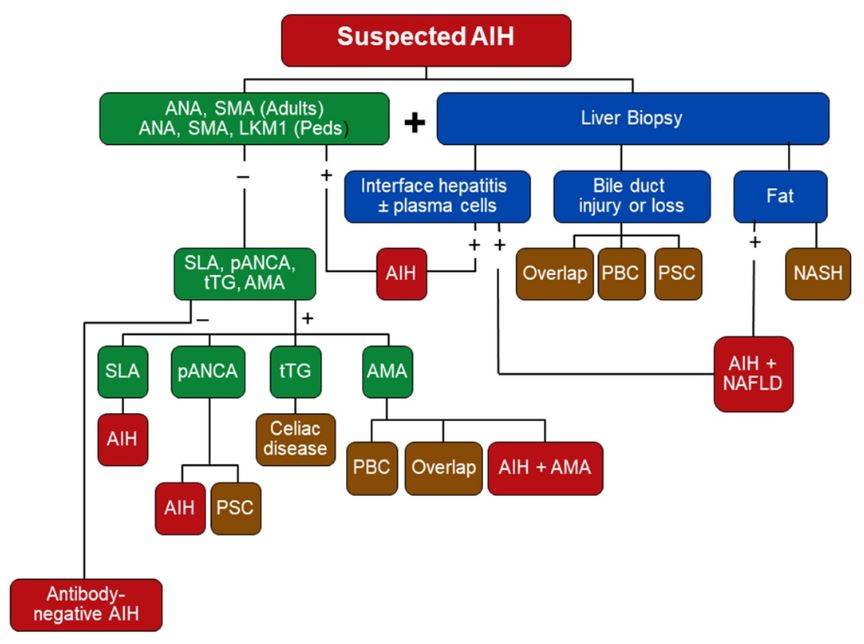
| Classic Autoantibodies (20% of AIH can be negative for ANA, SMA, LKM) |
ANA
(antinuclear Ab) and/or SMA (Smooth muscle Ab) / Antiactin Ab |
LKM1 (Liver
Kidney Microsome Type 1 Ab) (usually without ANA or SMA Ab) |
| Additional Autoantibodies |
SLA (Soluble Liver antigen) (20%) pANCA (50-92%) - lack sensitivity Anti-actin (Filimentous actin Ab) subset of SMA Alpha-actinin Ab (66%) |
LC1 (Liver cytosol Type 1 Ab)
(32%) LKM3 (17%) |
| Immunoglobulins |
+/- Hypergammaglobulinemia |
IgA levels may be reduced |
| Presentation (More common) Can present as either |
Asymptomatic Chronic / Insidious onset Cirrhosis on Biopsy |
Acute onset ALF / Fulminant Hepatitis Earlier onset/more severe/difficult to treat |
| Age at Diagnosis 2 peaks:(10-20) & (45-70) |
adolescents and adults 80% of adult cases are type I |
< age 14 |
| Concurrent autoimmune Dz (occurs frequenly in both types) |
Autoimmune thyroiditis Rheumatic disease Celiac IBD |
Autoimmune thyroiditis Diabetes Autoimmune skin diseases (vitiligo, leucocytoclastic vasculitis, urticaria, alopecia areata) Celiac |
| Overlap with: PSC (Adults) ASC (Peds) |
Autoimmune sclerosing
cholangitis common Atypical pANCA positive Adults can have overlap with PBC (not peds) |
Rare to have ASC overlap Atypical pANCA negative |
| Remission after drug withdrawal |
Possible |
Rare Lifelong treatment required |