Category
|
Location
|
Patient
Symptomatic?
|
Timing
|
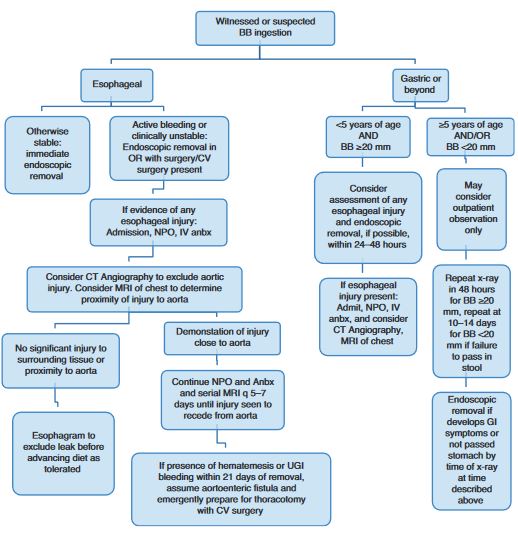
Button Battery
|
Esophagus
|
Yes or No
|
Emergent
|
|
Gastric/SB
|
YES
|
Emergent
|
|
|
No
|
Urgent - if Age < 5 and BB
> 20mm
|
|
|
|
Elective - if not moving on
serial films after 48hrs
|
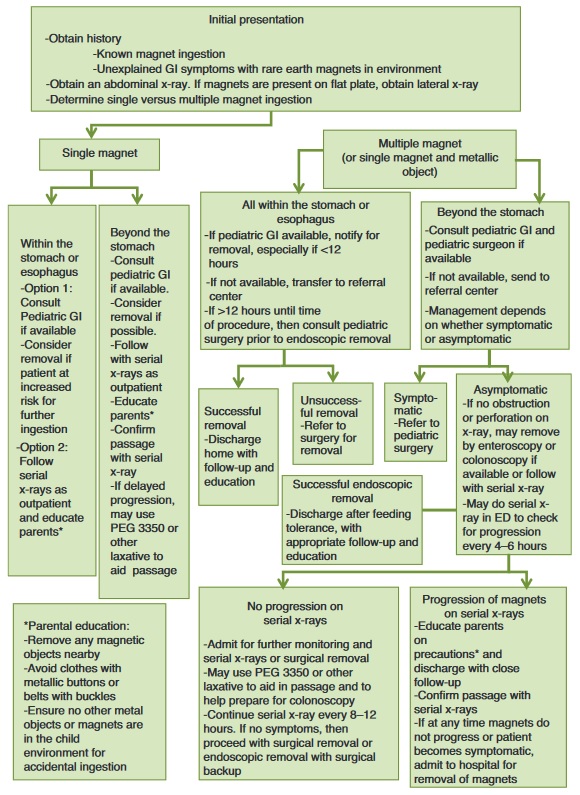
Magnets
|
Esophagus
|
YES
|
Emergent - if
not managing secretions (otherwise Urgent)
|
|
|
No
|
Urgent
|
|
Gastric/SB
|
YES
|
Emergent
|
|
|
No
|
Urgent
|
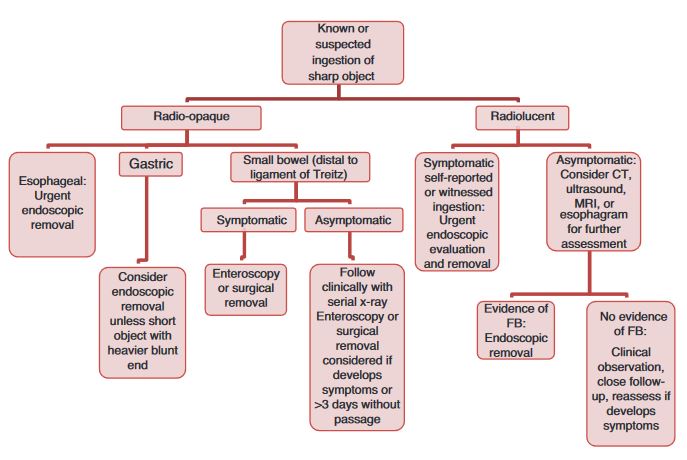
Sharp
|
Esophagus
|
YES
|
Emergent - if
not managing secretions (otherwise Urgent) |
|
|
No
|
Urgent
|
|
Gastric/SB
|
YES
|
Emergent - if
signs of Perforation, then Surgery
|
|
|
No
|
Urgent
|
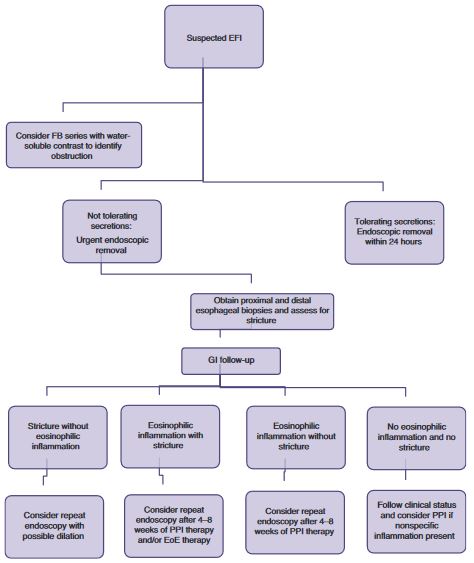
Food Impaction
|
Esophagus
|
YES
|
Emergent - if
not managing secretions (otherwise Urgent) |
|
|
No
|
Urgent
|
Coin
|
Esophagus
|
YES
|
Emergent - if
not managing secretions (otherwise Urgent) |
|
|
No
|
Urgent
|
|
Gastric/SB
|
YES
|
Urgent
|
|
|
No
|
Elective
|
Long Object
|
Esophagus
|
YES or No
|
Urgent
|
|
Gastric/SB
|
YES or No
|
Urgent
|
Absorptive Object
|
Esophagus
|
YES
|
Emergent -
if not managing secretions (otherwise Urgent) |
|
|
No
|
Urgent
|
|
Gastric/SB
|
YES or No
|
Urgent
|